“PK Band” in Laparoscopic Hernia Repair

Ramakrishnapillai, P., Gupta, S., Pai, M. et al. “PK Band” in Laparoscopic Hernia Repair. Indian J Surg (2020). https://doi.org/10.1007/s12262-020-02088-z
Abstract
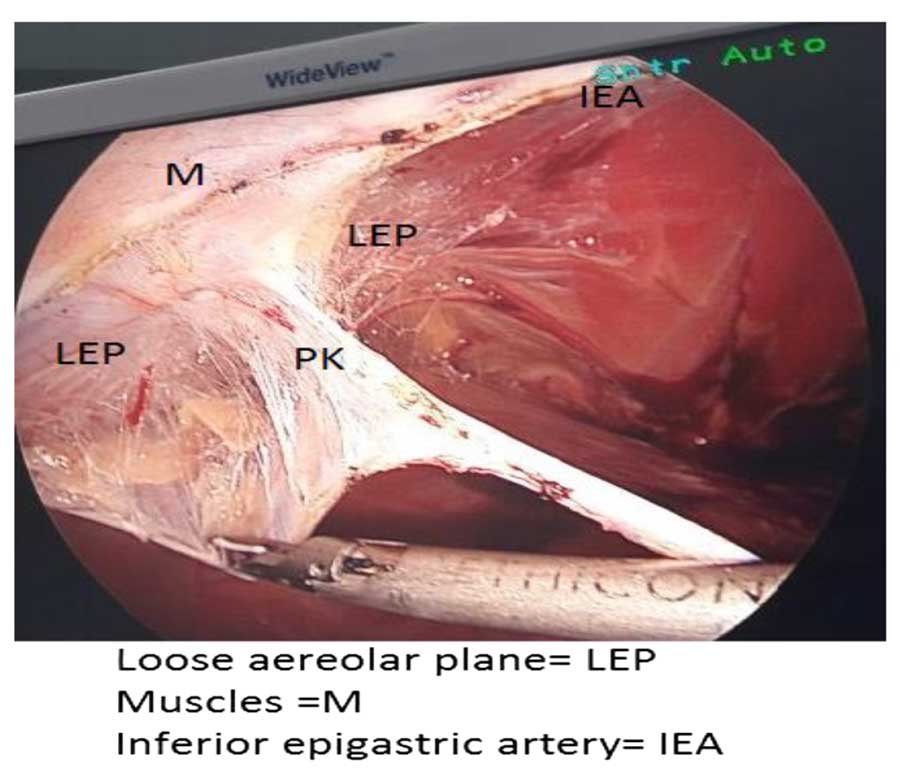
Laparoscopic inguinal anatomy detail is different from that is necessary for open hernia surgery. ‘PK Band’ is a condensation of areolar tissue lateral to inferior epigastric vessels on either side. It extends fromarcuate line to apex of triangle of doom. It is more condensed and prominent in the upper part. ‘PK Band’ is more prominent in males and tall structured individuals. It is an important land mark during laparoscopic inguinal dissection in both TEP (total extra peritoneal) and TAPP (trans abdominal preperitoneal) methods. Lateral blunt dissection in the preperitoneal plane will definitely be restricted by this band. Forcing the scope laterally will cause tear of the peritoneum at that level. Muscle injury may also be caused by blunt dissection. Division of this band during laparoscopic hernia repair connects the space of Bogros with space of Retzius. This provides sufficient space necessary for proper placement of mesh and hence significantly reduce recurrence.
Keywords : ‘PKBand’ . Laparoscopy . Inguinal Hernia . TAPP . TEP . Facia Condensation
Watch Video Presentation in YouTube
Watch in YouTubeConflict of Interest
None
Introduction
This is an observational information where we attempt to explain the anatomical importance and clinical significance of “PK Band” which is a fibrous band encountered while performing cases of laparoscopic inguinal hernia repair. During our 20 years of experience in performing over 6000 cases of laparoscopic hernia repairs, we made this observation. Identification of this structure is necessary for proper dissection and comfortable placement of mesh during laparoscopic inguinal hernia surgery.
Background
Nyhus et al. (in 1991) [1] have mentioned about transversalis fascia analogues [2, 3]. In the endoabdominal fascial sac, there are several locations of condensation of the fascia, which are continuous with and integrated to the sac itself.
These condensations, termed as transversalis fascia analogues, are found at points of insertion of various muscles or at points where aponeurotic structures are attached to the fascial sac. The five important fascial analogues are transversalis fascial sling, transversus abdominis aponeurotic arch, the iliopubic tract, iliopectineal ligament, and the interfoveolar ligament.
There is mention of medial boundary of Bogros space as a condensed area lateral to inferior epigastric vessel [4]. Also, there is mention of lateral boundary of Retzius space as condensation of tissue lateral to inferior epigastric vessel. But the surgical importance of this thickened area was not evaluated or described probably because it may not be important in open hernia surgery.
Location of the ‘PK Band’
The “PK band” is a condensation of the loose areolar tissue between the space of Bogros and the space of Retzius. It lies lateral to the inferior epigastric artery bilaterally. It extends from the arcuate line to the apex of the triangle of doom. It is more condensed and prominent in the upper part.


Prevalence of PK Band
It is seen in all patients. More prominent in males, tall statured and in well-built individuals.
Significance in Laparoscopic Hernia Repair
1. In totally extraperitoneal (TEP) repair
For surgeons, the lateral blunt dissection in the preperitoneal plane will definitely be restricted by this band. Forcing the scope laterally will cause tear of the peritoneum at that level. Extraperitoneal space is lost and the operating surgeon will not be able to complete a good lateral dissection. The procedure may have to be converted to intraperitoneal approach or open surgery due to air leak into the general peritoneal cavity. Many surgeons limit the lateral dissection to this band and place the mesh improperly. The principle behind mesh placement is that it should be placed equidistant laterally and medially to the inferior epigastric artery so that it adequately covers the indirect and direct hernial defects. Mesh placed without lateral dissection will not be covering the indirect hernia defect. Mesh folding can occur and it may lead to recurrence of hernia [5]. To prevent all these lapses during surgery and to avoid unnecessary delay and difficulty in dissection, the surgeon should divide “PK Band.”
2. In transabdominal preperitoneal (TAPP) repair
While dissecting in the loose areolar plane for placement of mesh, “PK band” is the landmark which is encountered lateral to the inferior epigastric artery. There is loose areolar tissue on either side of this band. In order to complete lateral dissection for smooth placement of mesh, it is imperative that just as in TEP the surgeon divides “PK Band.” If not identified, there is strong possibility for either peritoneal tear or injury to the muscles, and mesh placement will be improper leading to recurrence of hernia.
Conclusion
“PK Band” acts as an important anatomical landmark in both TAPP and TEP. Its division is necessary in proper completion of lateral dissection and proper placement of mesh.
References
- Nyhus LM, KleinMS, Rogers FB, et al. (1991) Current problems in surgery. 28(6):407–450. doi: https://doi.org/10.1016/0011-38
- MemonMA, Quinn THet al (1999) J Laparoendosc Adv Surg Techn 9(3):267–272. https://doi.org/10.1089/lap.1999.9.267
- Annibali R., Fitzgibbons R.J. (1995) Laparoscopic Anatomy of the Abdominal Wall. In: Phillips E.H., Rosenthal R.J. (eds) Operative Strategies in Laparoscopic Surgery. Springer, Berlin, Heidelberg
- Ansari MM, et al. (2017) Retzius and Bogros spaces: a prospective laparoscopic study and current perspectives.Ann IntMedDental Res 3(5)
- Choy C, Shapiro K, Patel S et al (2004) Surg Endosc 18:523. https://doi.org/10.1007/s00464-003-8183-0
Author information
Affiliations
- Department of General & Laparoscopic Surgery, VPS Lakeshore Hospital, Kochi, India
- Padmakumar Ramakrishnapillai
- , Sandeep Gupta
- , Madhukara Pai
- , Aravind Balakrishnan
- , Kevin J Chiramel
- & Premna Subin
- VSM Hospital, Mavelikkara, India
- Farish Shams
- Verwandeln Institute, Kochi, Kerala, 682306, India
- Subin Thomas
Lap Hernia Repair in Detail
About Dr. R. Padmakumar
Dr. R. Padmakumar is one of the Best Hernia Surgeon in India. He has been changing lives through Keyhole Surgery. He has got more than 30 years of hands-on experience in laparoscopic Surgery in major hospitals across India and has completed more than 7000 cases of Laparoscopic Hernia Surgeries. Dr. Padmakumar has trained more than 300 surgeons from all over the world the art of laparoscopic surgery especially Laparoscopic Hernia Surgery. Dr. Padmakumar is also hailed as one of the Best Bariatric Surgeon in India & UAE. He is renowned for new and improved treatment techniques and the first in the World to perform Scarless Bariatric Surgery with Tummy Tuck / Abdominoplasty. He is also one of the very few thyroid surgeons in India doing Endoscopic Thyroidectomy (scarless thyroid surgery).



-
Anal Fissure Treatment
-
Gynaecomastia Treatment
- Piles / Hemorrhoids Treatment
- Varicose Veins Treatment
- Laser Treatment for Varicose Veins
- Diabetic Foot Treatment